

By Ron Conte, Pharm.D.

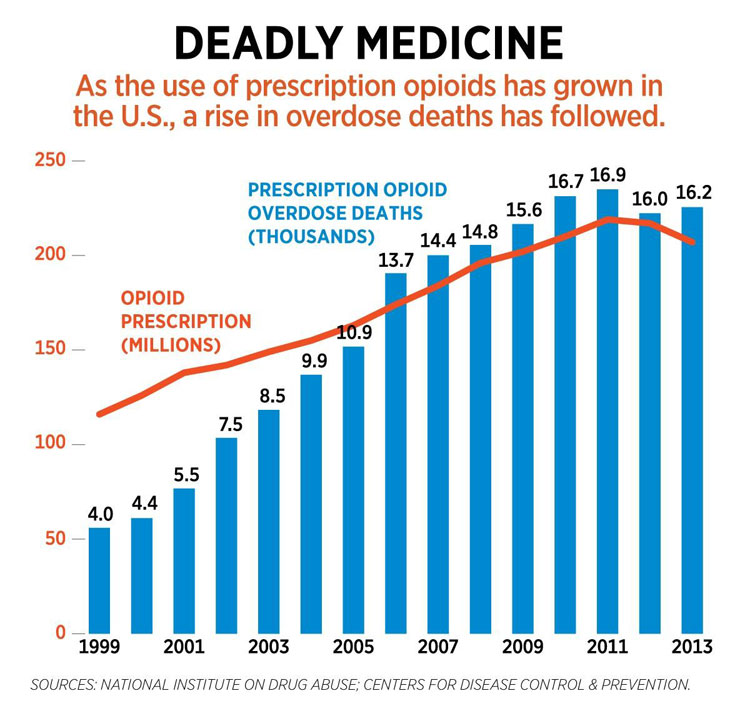
From recent accounts, 115 Americans die every day from an overdose of opioids. In 2015, two million Americans were labeled as having an opioid disorder, meaning these individuals took an opioid for non-medical purposes. Almost 30% are classified specifically as having a heroin use disorder. Heroin is an illegal substance in the U.S. How we got to these epidemic numbers is somewhat complex, involving many factors. I will touch upon a few of them, however it is important to start with a basic understanding of opioid effects.
![]()
Narcotics can be administered by mouth (orally, including under the tongue), subcutaneously (under the skin), transdermally (through the skin by use of a patch), intramuscularly (into a muscle), intravenously (into a vein), epidurally (through a space in the spinal cord), intrathecally (within the cerebrospinal fluid), and intra-articularly (into a knee or shoulder joint). Depending on which narcotic is administered and by which route, the time to onset of pain relief differs.
Recent studies show an increase in opioid-induced pneumococcal infections of the lungs that can be quite severe and sometimes fatal. Other narcotic effects include a decrease in blood pressure, constipation, nausea, vomiting, urinary bladder dysfunction, itching, muscle rigidity, and pinpoint pupils of the eyes. If a patient develops a tolerance to a narcotic, the drug may even cause dysphoria (a feeling of dissatisfaction with life).
One factor leading to the opioid crisis is prescribing narcotics for pain that can be treated effectively with non-narcotic agents. Non-narcotic pain relievers include acetaminophen, NSAIDs (Motrin and others), as well as antidepressants (Elavil and others), and anticonvulsants (gabapentin and Lyrica).
There is actually a “stepped-care” approach for treating types of pain. To treat pain quickly and effectively, the origin of pain, location of pain, and whether pain is acute or chronic are important to know. So, for example, nerve pain as in sciatica, may best be treated with an antidepressant. In fact, narcotics are minimally effective in treating nerve pain, fibromyalgia, headaches, low back pain, jaw pain, and irritable bowel syndrome.
A second factor leading to the opioid crisis is in part due to use of long-acting narcotics when short-acting agents will suffice. There is no proof that long acting narcotics are safer or more effective. The risk of overdose is two-times greater with long acting than with shorter acting narcotics.
•••
In my next article (Part II), I will discuss a few other factors contributing to the opioid crisis. I will also discuss a three-pronged approach to deal with the crisis.